Who to track?
• Man aged 65 to 75 smoker (defined as a minimum of one cigarette / day) or former smoker (defined as having stopped smoking for less than 20 years regardless of the number of cigarettes consumed) .
• Male aged 50 to 75 with a family history at the first degree of AAA (father, mother, brother or sister).
Which screening tool?
• Aortic arterial echo-Doppler and lower limbs performed by a vascular physician.
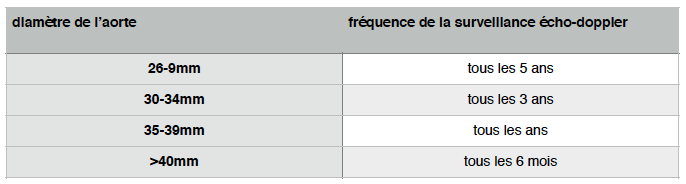
What pace of surveillance?
Surveillance should be performed by the attending physician and paraclinic by an arterial doppler echo of the lower limbs to be performed by a vascular physician.
What general care should be provided by the attending physician?
• Offer tobacco cessation assistance.
• Normalize blood pressure (note that beta-blockers do not alter the course of AAA).
• Encourage regular physical activity.
• Reduction of hypercholesterolemia.
• Reduced overweight.
• Control pre-existing diabetes.
In practice:
• Introduction of a statin, as it reduces perioperative mortality (recommendation A).
• Use of beta-blockers does not limit the evolution of the aortic aneurysms. They are useful however in patients with high risk of cardiovascular disease in pre-operative (recommendation A).
• The use of low-dose antiplatelet agents (aspegic 250mg) is beneficial for patients with aortic aneurysm, especially if the patient has atherosclerotic arterial disease (recommendation A).
• No specific recommendations for ACE inhibitors or ARBs 2 in patients with aortic aneurysms.
When to operate?
The consensus is to operate the renal abdominal aortic aneurysms of more than 5cm.
At less than 4.5 cm in diameter, the risk of rupture is less than 1% per year. It is not appropriate to propose preventive treatment before breaking before 5 cm.
In some cases it is advisable to discuss earlier treatment:
• Symptomatic iliac occlusive lesions associated
• iliac aneurysmal lesions greater than 3 cm.
• Rapid growth of more than 1cm / year.
• Saccharum aneurysm
In general, large aneurysms increase diameter more rapidly than small aneurysms. The aneurysms of 3 to 3.9 cm in diameter increase on average by 0.53 cm per year and those of more than 6 cm by 0.8 cm per year. Whether considered as linear or exponential, this growth exposes the risk of rupture. This risk is higher the larger the diameter of the aneurysm.

Who to operate?
Any patient with an aneurysm greater than 5 cm. This is to be weighed by the following elements:
• The short-term benefit of treating aortic aneurysms for patients with a life expectancy of less than 3 years seems uncertain.
• In patients with a life expectancy of less than 3 years, the benefit of the treatment of an abdominal aortic aneurysm must therefore be « discussed » on a case-by-case basis by all the participants around the patient (treating physician, geriatrician, surgeon …).
• In patients with good life expectancy but with high operative risk:
◦ wait 6 cm or if the aneurysm is symptomatic.
◦ or use a minimally invasive endovascular technique if the anatomy of the patient allows.
What treatment to propose?
Three surgical treatments can be proposed:
• Conventional surgical treatment by laparotomy.
• Endovascular treatment.
• Laparoscopic or robotic treatment.
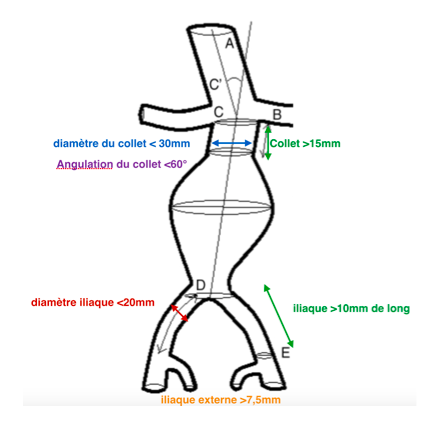
The endovascular treatment can only be proposed if the anatomical conditions of the patient allow it, namely:
What follow-up?
For life. The follow-up is useful for the detection of complications due to the surgical treatment but also to the detection of the associated aneurysmal pathologies (popliteal aneurysm …)
This monitoring depends on the type of treatment.
- In the case of conventional or laparoscopic surgical treatment: annual arterial echo-doppler monitoring (detect associated aneurysms: poplites, iliac …, absence of false anastomotic aneurysm).
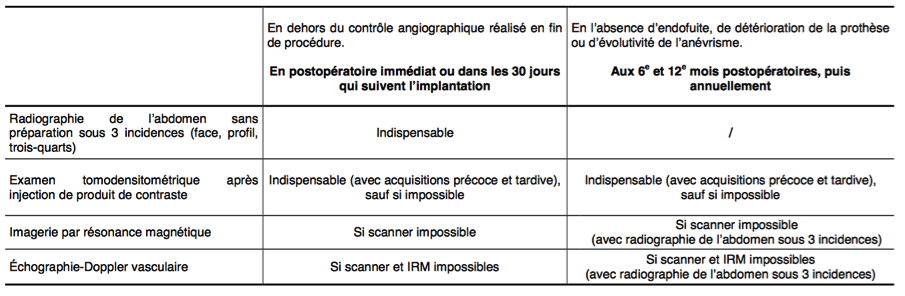
- In case of endovascular treatment: a strict schedule must be followed for the follow-up of a stent.
Sources:
Has: http://www.has-sante.fr/portail/upload/docs/application/pdf/2013-02/aaa_fiche_med_vfinale.pdf
European Society of Vascular Surgery: http://www.lfb.lv/files/ESVS-AAA-guidelines.pdf
French College of Vascular Surgery: http://www.cfcv.fr/reperes.htm